Michael Coburn, MD, FACS, presented “Management of High Grade Renal Trauma” during the 23rd Annual Innovations in Urologic Practice on September 14, 2018 in Santa Fe, New Mexico.
How to cite: Coburn, Michael. “Management of High Grade Renal Trauma” September 14, 2018. Accessed [date today]. https://dev.grandroundsinurology.com/urethral-strictures-guidelines-update/
Management of High Grade Renal Trauma – Summary:
Michael Coburn, MD, FACS, discusses decision-making for urologists consulted in kidney trauma cases. He defines indications for active observation, nephrectomy, and non-operative interventions, as well as practical techniques for gaining vascular control and reconstruction.
Abstract:
The approach for most kidney trauma cases is observation and non-operative management. However, for certain patients, non-intervention could be harmful. When consulted for a kidney trauma case, urologists must determine the threshold at which a patient should shift from active observation to an interventional option.
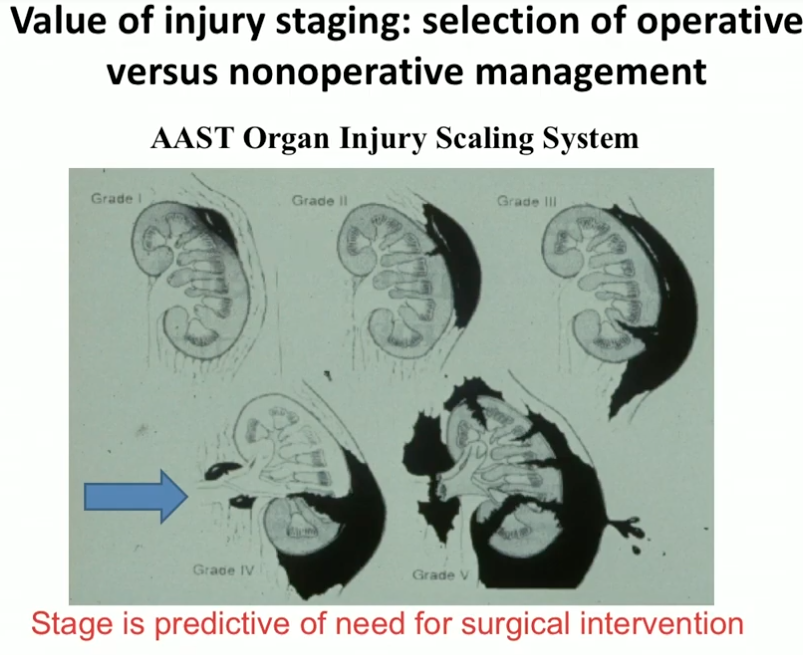
The American Association for the Surgery of Trauma (AAST) Organ Injury Scaling System is an important predictive factor of need for surgical intervention. Injuries classified as Grade I-III only require careful observation, while those classified as Grade IV-V are likely to require intervention. Grade IV injuries in hemodynamically stable patients are also reasonable candidates for observation.
During trauma laparotomy, indications for exploratory surgery in the kidney include expanding hematoma, brisk bleeding into the peritoneal cavity, and high risk for nonoperative management shown on computed tomography (CT) scan. Otherwise, it is appropriate to delay exploration until postoperative CT staging provides definitive information. When CT shows solitary renal injury but there is no planned trauma laparotomy, urologists should consider exploration or nephrectomy for Grade V injuries. Grade IV injuries in this situation could be appropriate candidates for interventional radiology (IR).
In instances in which patients require operation, clinicians must rapidly gain pedicle access and control, expose and mobilize the kidney, and evacuate the hematoma. This presentation provides detailed practical instructions for achieving these steps, including the “pedicle access maneuver.” After this, it is essential to make a key decision point as to whether it is possible and feasible to salvage the kidney given the patient’s overall clinical condition, or to proceed with nephrectomy, early in the process. Clinicians must also consider and be familiar with indications for nonoperative IR or endourologic intervention in these cases. When monitoring during non-operative or postoperative care, clinicians must still define a threshold and strategy for moving to intervention.
About Innovations in Urologic Practice
Innovations in Urologic Practice (IUP) is an annual CME-accredited conference devoted to updating urologists on the rapidly changing healthcare environment. Topics focus on innovative diagnostic and treatment strategies, controversies, new and currently developing technologies, and challenges in today’s urologic practice. Dr. Coburn presented this lecture during the 23rd IUP in 2018. Please visit this page in order to learn more about future IUP meetings.