Dr. Ryan P. Terlecki presented “Erectile Dysfunction and the Detection of Subclinical Cardiovascular Disease” at the 26th Annual Perspectives in Urology: Point-Counterpoint, November 10, 2017 in Scottsdale, AZ
How to cite: Terlecki, Ryan P. “Erectile Dysfunction and the Detection of Subclinical Cardiovascular Disease” November 10, 2017. Accessed Dec 2024. https://dev.grandroundsinurology.com/erectile-dysfunction-detection-subclinical-cardiovascular-disease
Summary:
Dr. Ryan P. Terlecki, MD, FACS, reviews the data linking erectile dysfunction and cardiovascular health, data on the potential risks with standard medications that are commonly used, and discusses the steps in evaluating a patient before he is put on PDE5 inhibitors.
Erectile Dysfunction and the Detection of Subclinical Cardiovascular Disease
Transcript:
ED and the Detection Subclinical CVD – Ryan P. Terlecki, MD, FACS
Alright. Well, it’s after lunch so hopefully we can fight some of that postprandial somnolence and keep it rolling. Nothing should wake you up more than a discussion about sex, right? So let’s see, can we cue up the slides, please.
This is a very salient topic, right? Talking about cardiovascular risk, and the patients coming to you for their sexual health. So I’m going to go over not only that connection, a little bit inside our medical management. How many people by show of hands treat ED in their clinical practice? Okay, so most of you. So it’s not just cancer that we’re talking about in the course of this meeting
Disclosure of Financial Relationships
Again my disclosures.
Objectives
Objectives. Go over the data linking the two conditions, ED and cardiovascular health. Look at the steps in evaluating the patient who comes to your office before you start them on PDE5 inhibitors; and the opportunities for lifestyle modifications; and some data on potential risks with these standard medications we often use.
Regarding management of erectile dysfunction, which of the following is TRUE?
So audience response question. Regarding PDE5 inhibitors for management of ED, which if the following is true? A causal relationship has been established between PDE5Is and melanoma; sildenafil should be avoided in renal transplant patients; PDE5Is have been shown to reduce recurrence rates of prostate cancer; daily tadalafil is not recommended for dialysis patients; nitrate use is no longer contraindicated for men using PDE5Is.
With only 16 responses, yeah, we’re spread out. So this gives us an opportunity for some education.
Which of the following classes of medication are not believed to?
Let’s go onto our next one.
Which of the following classes of medication are not believed to adversely affect erectile function? Antiarrhythmics; tricyclics; thiazides; beta blockers; or calcium channel blockers?
Awesome, okay. This will be good.
Relevance
So ED is seen in the majority of men over the age of 40. It doesn’t mean it’s severe in everybody, but over half of men between the ages of 40 and 70 have some degree of ED and that was based on the Massachusetts Male Aging study, but nearly 20% of all men have moderate to severe ED, and this compromises quality of life, not only for men, but for their partners as well. And it can lead to loss of compliance and adherence to treatment. ED may be the sentinel symptom in those patients with undiagnosed peripheral or coronary artery disease. So it’s like the canary in the coal mine, right? You go down, if you want to know something is amiss early, you take the bird, carbon monoxide kills the canary before it kills the miner.
Canary in the Coal Mine
Francesco Montorsi in Italy looked at 300 consecutive angina patients coming to the ER with chest pain, who had angiography confirming coronary artery disease, nearly half had ED. So looking at those patients they had both heart disease and ED. Two-thirds of them had their ED symptoms prior to chest pain with a mean interval of about three years and change.
PCPT Data
Ian Thompson, looked at the PCPT data. He had men that were 55 and over, almost 10,000 in the placebo group, and they were checking them every three months for their sexual function and cardiovascular disease for a prolonged period of time. Prevalent or subsequent incident ED after five years was significantly associated with subsequent cardiovascular events. And that was found to be on par with smoking or a family history of myocardial infarction.
Olmsted County Study
A colleague of mine, Brant Inman over at Duke, looked at the Olmsted County data. This was a great paper. And he looked at the association between the ED and the long-term risk of developing heart disease. He looked at age as a modifier, and for a man below the age of 50, having ED was associated with a 50-fold increase in the incidence of heart disease.
Younger Patients = Red Flag
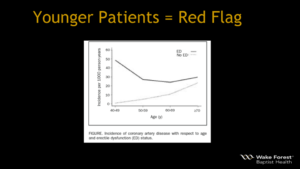
Here that is, this is represented graphically, and again you have age here, okay. But if you look at a guy, and you could certainly see a multiple choice question, if you had a guy coming in 48, 49 years old with ED, his rate of heart disease compared to somebody without it, 50-fold higher.
Mayo Data (Kopecky’s group)
Steve Kopecky who is a cardiologist at Mayo, I saw him recently at the SMS meeting. His group did a prospective study of over 1,000 men in that same age range I mentioned to you before. Mean follow-up was over 11 years and they had 261 new cases. ED was significantly associated with cardiovascular disease even after controlling for age, and associated risk factors, and their Framingham score. However, it didn’t improve prediction of cardiovascular disease beyond traditional risk factors, but a lot of us in urologic practice aren’t looking at those traditional risk factors as well as some other physician might be.
Initial Evaluation: History
So what do you do? Well you take your standard history of course. We talk about libido, that primal urge to pursue sexual activity, but sometimes if that’s down, it could be a compensatory mechanism for loss of function. Guys don’t want to start something they can’t finish so sometimes they withdraw, right? There’s ejaculation disorders, orgasmic disorders, structural disorders, and the setting of Petronie’s disease. A SHIM questionnaire, we’ve talked a little bit about questionnaires in the course of this meeting, like when we were asking Matt about why don’t you use an AUA symptom score. Well time’s the answer, because there’s so many questionnaires out there. Some people will get these things filled out in their office at a urology clinic, and they never read them. They’ll get put in electronically, and perhaps by nursing, and then they just fall by the wayside. We have published though that you can ask just a single question, and it’s still a good screen. So certainly look at lifestyle and reversible causes.
Simple Screen for Potential CVD
A simple screen for potential cardiovascular disease, two questions. One, do you have any chest discomfort or shortness of breath with exertion? And if so, does it bet better with rest? Simple. You can do that.
Medication-Induced
What about medication induced ED? We’re all pretty well familiar with the beta blocker effect. A lot of blood pressure meds can cause that. However, ACE inhibitors, angiotensin receptor blockers, and calcium channel blockers have either a neutral or beneficial effect. There’s also the possibility of the Hawthorne effect where is a patient knows that this can cause ED, he thinks he has ED. Antiandrogens, antiarrhythmics can cause ED. Statins however a little bit controversial, but most of the data suggest they may actually be beneficial for patients with ED.
Initial Evaluation: Physical
Next slide. Alright, physical exam. So one of the things we talk about in addition to vitals is waist circumference. And this is important because this is used in certain model to determine cardiovascular risk. Of course you can look at the traditional items, I’ll admit I don’t have a stethoscope in my office. Some people do, they’ll still carry it around. Testicular exam, certainly if you’re looking at for signs of endocrine issues, if you have atrophy. Plaques of course if you’re looking for anything related to curvature. And then signs suggesting vascular or neurological disease.
Lab testing (optional)
Lab testing is considered optional in the workup of a man with ED. However, a fasting glucose, we talked about this earlier, is a good test. A1c plus or minus, I do that before any surgical, elective surgical case in my practice. Lipid profiles are valuable if you’re going to do risk scoring, and it’s not that hard to do that and I’ll show you that in a second. CBC, CRP, again, reasonable to consider but not mandatory by any means. Hormone profiles are somewhat controversial, however, certain guidelines do advocate checking testosterone especially if they fail oral medications for first line therapy. I may check estradiol, especially if we have someone who is obese. And then I look at a pituitary panel as well.
Specialized testing
Specialized testing, now who here does penile duplex in practice? Nobody.
Alright, good, so I’m not going to offend anybody. I don’t really do that a whole lot because I don’t feel it changes management, okay? It can however provide some kind of cognitive or psychological benefit to the patient. No one really does nocturnal penile tumescence anymore, it had poor correlation with the SHIM score and it’s obviated by good history and physical. Psychological evaluation, it doesn’t necessarily have to involve certain inventories in questionnaires, but you kind of get a sense of what’s going on with the patient when they come to you for their sexual health. Neurophysiologic testing, again doesn’t assess autonomics, and it’s time consuming. Arteriography seems way overboard. EndoPAT, we published previously in Journal of Urology, it’s the only FDA approved noninvasive test for endothelial dysfunction.
Erectile Dysfunction is Predictive of Endothelial Dysfunction in a Well Visit Population
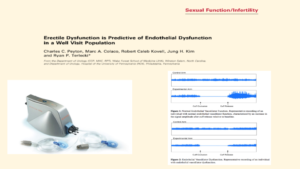
And so this was something that can be done quickly in the office. It generates a score, and depending on the results, you can decide if the patient warrants a subsequent next level testing with the cardiologist. It reimburses fairly well, and it’s easy to do in your clinic.
Penile Duplex
As I mentioned, bottom line on this slide you can see in the bold, is that the penile duplex may provide information that the patient understand, again not changing management, however, I don’t know if this really comes up on exams if you don’t do a lot of ED for research, but peak systolic velocity above 30 cm/s is considered normal; less than 25 cm/s suggest arterial insufficiency, then you look at end diastolic volume. If it’s above 5 cm/s it suggests venous leak, but you can only diagnose it if they have normal arterial function. So that could be somewhat problematic. So remember the male sexual response is pretty complex.
How it works
I never tell any man who comes to my office that it’s all in your head. But I’ll tell every man whoever had had a problem with his erection, that there’s always a psychological component, because their always wondering how is it going to be for me this time? And sometimes when they should be enjoying sexual activity, they’re kind of checking themselves out, thinking how am I doing? So you have the nerve component, the blood flow component, the hormone component which we heard about earlier as well, but you need to intact vascular endothelium. The nerves are stimulated, acetylcholine, and the release of nitric oxide, and then cyclic GMP, and then ultimately you get flow. Oxidative stress, we talk a lot about. Patients especially now are coming in asking about antioxidants and natural therapies. The reactive oxygen species that are generated by different diseases or medications lead to endothelial dysfunction, and reduce release of nitric oxide.
Link to CVD
Endothelial dysfunction seems to be the common link to cardiovascular disease in patients with ED. And this can be improved by weight loss, and increased activity, and we’ve seen this in studies showing changes in markers of inflammation, like IL-6, and C-reactive protein. Drugs like statins, as I already mentioned, but also some of these others listed here have been shown to improve endothelial dysfunction. And phosphodiesterase inhibitors may do so as well.
ED and the Heart
Chicken or the egg, right? So heart disease can be a cause of ED, or it could be a product of the same underlying issue. Similarly, a lot of the medications these men are on, may be detrimental to their sexual function. However, if you can effectively treat their sexual dysfunction, you can lessen their anxiety, possibly preventing worsening of their heart disease, and improving upon their quality of life. Chest pain during intercourse which represents only a small percentage of all chest pain encounters can lead to avoidance of sexual activity and decreased quality of life, and this has been published.
ED and the Heart
The Princeton III panel said that all men presenting with ED should be assessed for their cardiovascular risk. What does that mean for you? Does that mean that you have to do intensive screening in your office? No. And does it mean you have to do a Framingham score? No. But you should assess these patients. If they are at low risk, again risk factor management. If they’re high risk, get them over to a cardiologist. And because there’s so much overlap between what we do in internal medicine and the endocrinologist and the cardiologist, it creates a nice work group to really identify men at risk, and that would benefit from your services. The intermediate risk group probably warrants evaluation with either exercise, stress testing, or some other means. Phosphodiesterase inhibitors do not reduce exercise tolerance, or increase events in men with heart disease. If a guy comes and he’s not on any nitrates, if he’s healthy enough to walk in and out of your office, and you don’t see any other contraindications, just the fact that he has a history of heart disease doesn’t mean that he can’t have medications for his sexual health. However, Avanafil which I don’t typically prescribe is not recommended in those who have had an event within the past six months, so if you so use that drug, you should be aware.
Framingham Risk Score Calculator for Coronary Heart Disease
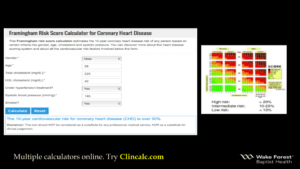
I filled out these numbers. I don’t know how well they project because it’s a little dim, okay. But there are multiple online risk calculators. If you have a smart phone and you carry it with you in your office, you can always just type in this website, clincalc.com. Literally it will take you 60 seconds to calculate this man’s risk if you have these values. Gender, male; age, in this one I put in 58; total cholesterol; HDL. And so you’ll get asked question about their hypertension and their systolic blood pressure, and if they’re a smoker. You hit calculate. In this scenario, the 10-year cardiovascular risk for heart disease is over 30%, so that’s important.
Bottom Line
Bottom line, if you’re going to prescribe a tablet, you should check their cardiovascular risk. If you treat ED upfront successfully with meds and the patient just comes back once a year for refills but doesn’t address his lifestyle, have you hurt him? There’s a lot of guys that come to me that don’t even have a primary care doctor, and the only reason that they even went to see a provider is because they want better sexual function. Sometimes by not looking deeper, I would compare it to treating a bleeding chest wound with a red sweater. So get you to the party, but you won’t be partying long.
Lifestyle Modifications
What about lifestyle modifications? We talk a lot about it. Matt talked about this earlier, but it’s easier said than done, right? Somebody made a comment, how many of your patients go to the gym for example, to try to boost testosterone? How many of you in the audience have ever tried to lose weight or change your diet, or say you’re going to get to the gym, and then not do it? Lots of us. So however, there was a randomized single blind trial looking at obese men with ED that found that detailed advice did result in a significant drop in BMI, and changes in their inflammatory markers. Their mean IIEF score improved by about 3 points, which was statistically significant but again keep that in perspective. On a multivariate analysis, changes in BMI, activity, and C reactive protein were independently associated with improvement in erectile function.
Lifestyle Modifications
 A meta-analysis of six clinical trials, again saw significant improvements in their IIEF score with lifestyle modification. And again, 2.3 to 2.6, which is pretty much less than one tablet of Viagra. It’s positive, but it’s not a homerun. Remember the whole comment I made before in terms of BPH symptoms, vasib [phonetic] versus homerun in terms of impact.
A meta-analysis of six clinical trials, again saw significant improvements in their IIEF score with lifestyle modification. And again, 2.3 to 2.6, which is pretty much less than one tablet of Viagra. It’s positive, but it’s not a homerun. Remember the whole comment I made before in terms of BPH symptoms, vasib [phonetic] versus homerun in terms of impact.
The holy grail
When Viagra came out, again, the game changed. It was originally investigated to treat angina. It had marginal benefit and had the peculiar side effect of improve erections. And then hit the scene in 1998 and then you had subsequent drugs follow. Some of these drugs you see at the bottom aren’t approved in the United States, but are available in places like Korea.
Other conditions treated
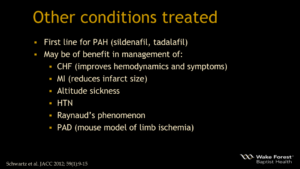
This class of medication is used for a variety of conditions. That’s why you can get generic sildenafil, not Revatio it’ll be listed as, pulmonary hypertension. But that’s why it only comes in the 20 mg tablets as well.
Pharmacokinetics
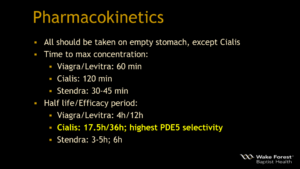
All of these drugs typically, except Cialis should be taken on an empty stomach and I’ve listed the time to maximum concentration. Even though they don’t necessarily have to wait that full amount of time to reap benefit. The half-life and efficacy is listed here, many of us are aware of this. Cialis you should know though has the highest selectivity for type 5 phosphodiesterase.
Which one is best?
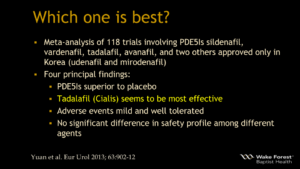
Which one is best? I would kind of encourage you not to just give someone prescriptions for all of these, or a bag of samples and say try them all and see what works best. That can be frustrating for men and sometimes it can have negative consequences. A meta-analysis of 118 trials had four principle findings. These drugs work better than nothing, well that’s not surprising. But Cialis seems to be the most effective. Adverse events are mild and well tolerated, and there’s no significant difference in safety profile among these different drugs. I tend to use Cialis more but again, with cost concerns a lot of us probably default to generic Viagra for many of these patients.
Mechanism of action
These drugs are structural analogs, so cyclic GMP. They bind to the catalytic site and inhibit hydrolysis. Cyclic GMP levels go up, raise penile blood flow, and amplify the neurologic signal.
Safety and Side effects
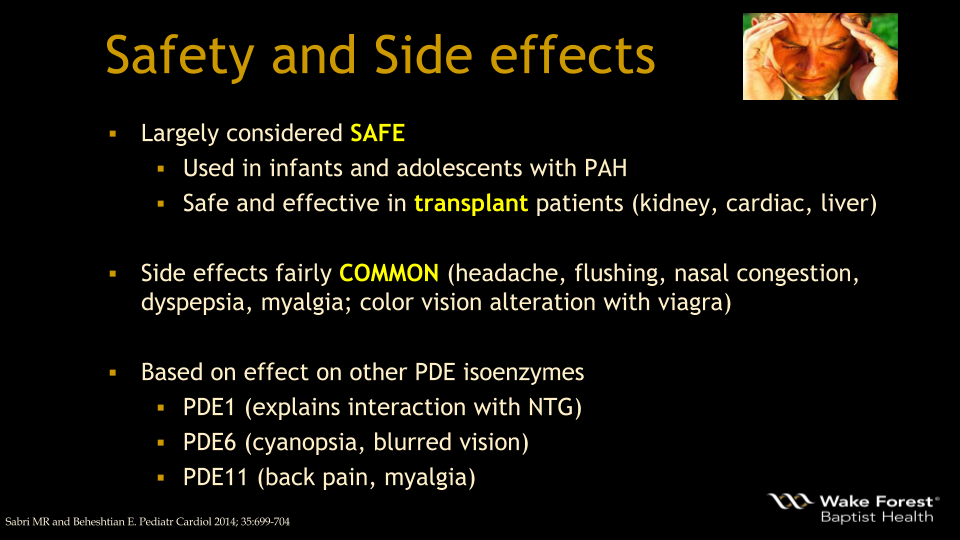 They are largely considered safe, they’ve been used in infants for their conditions. They are safe and effective in transplant patients and side effects are fairly common. Probably more common than what the drug inserts says because for those of us in practice, and many of you said you treat ED, headache, sinus congestion, these types of things, even in patients that are happy to keep using them will note that these happen. But I find that if you give a man a quality erection and he hasn’t had one in a while, he’ll overlook the headache or take a couple Tylenol before. The side effects are based on the effects with other isoenzymes of phosphodiesterase. Type 1, type 6, type 11, and you could see the side effects that we often discuss with patients listed there.
They are largely considered safe, they’ve been used in infants for their conditions. They are safe and effective in transplant patients and side effects are fairly common. Probably more common than what the drug inserts says because for those of us in practice, and many of you said you treat ED, headache, sinus congestion, these types of things, even in patients that are happy to keep using them will note that these happen. But I find that if you give a man a quality erection and he hasn’t had one in a while, he’ll overlook the headache or take a couple Tylenol before. The side effects are based on the effects with other isoenzymes of phosphodiesterase. Type 1, type 6, type 11, and you could see the side effects that we often discuss with patients listed there.
Safety: Renal patients
What about renal patients? You saw me ask a question about this before. ED is seen in overwhelming majority of dialysis patients, it affects their quality of life, and it’s seen in half of our transplant patients. Viagra will absorb faster after dialysis, and the max concentration of the half-life is increased by Prograf, which essentially all your kidney transplant patients are taking. Sildenafil is well tolerated in these patients, however, if the creatinine clearance is below 30, you should start at 25 mg. Looking at Cialis, if the creatinine clearance is 31 to 50, you start at 5 mg and a max dose of 10 mg, not the 20 mg. I find that a lot of providers have never heard this data before. If it’s less than 30, if they’re on dialysis, do not exceed 5 mg in 72 hours, this daily dosing is not recommended. Again, some of you are starting to think, oh jeez, I’ve probably got some of these patients, I never knew this before.
Chronic PDE5Is and the Heart
What about chronic use and the heart? Meta-analysis, 24 trials looking at efficacy and safety. Cardiac morphology and function was reported. The others concluded that these drugs have an anti-remodeling effect and they improved cardiac contractility with a good safety profile. And the ideal target population was felt to be those patients that had heart failure and left ventricular hypotrophy. It’s also been shown to be safe when given before bypass. Some people for a while they were saying we should put this in the water, right?
Chronic PDE5Is and Diabetes
Looking at diabetes, again it seems to have a positive impact and improves hemodynamic and serum pro-inflammatory markers in these men.
Nitrates
Nitrates are still contraindicated and implicated in some deaths. One group demonstrated that ranolazine could be used as a nitrate alternative, something for the patients to talk about with their cardiologist.
Other Drug-Drug Interactions
Remember if they are also on an alpha blocker, you want to separate the dose if it’s a non-selective alpha blocker. If it’s not, it’s not really an issue. Be aware if you’re using any adulterated supplements over the counter.
Melanoma Risk? US Data
What about melanoma? There was a study suggesting it induced melanoma invasion or with a hazard ratio of 1.8. And the rationale of meds acting similar to a proto-oncogene was reported, and increasing invasiveness by lowering expression of PDE5 type A.
Melanoma Risk? Swedish Data
There was a follow-up study to this, Swedish study and they looked at their melanoma registry, also showing an increased association.
Melanoma Risk: Data Critique
But it’s not necessarily cause and effect, and it may be related to socio-economic status and more exposure to sunlight. But we still don’t know. There might be a selection bias.
NAION
I don’t want to spend too much time on this based on our time constraints.
NAION 2
But in terms of NAION which is a form of optic neuropathy, the FDA has mandated a warning for this.
NAION 3
And subsequent studies that were commissioned to be performed by Pfizer did show that the odds ratio is real even though the absolute risk is still small.
NAION 4
So if the patients has a history of this, you want to exercise some caution.
Cancer Controversies
Cancer controversies. There was a German study suggesting it may increase biochemical recurrence which was actually opposite the hypothesis that they developed. The follow-up Italian study didn’t find the same thing. Both were retrospective, and the jury is still out.
Regarding phosphodiesterase-5-inhibitors for management of erectile dysfunction, which of the following is TRUE?
Alright, let’s go back to our questions before we close. Regarding the PDE5 inhibitors for management of ED, which of the following is true? Causes melanoma; should be avoided in transplants; it’s been shown to reduce prostate cancer recurrence; daily tadalafil is recommended for dialysis patients; or nitrates are not longer contraindicated.
Perfect. Almost perfect.
Which of the following classes of medication are not believed to adversely affect erectile function?
Next one. Which of the following classes are not believed to adversely affect erectile function? Antiarrhythmics; tricyclics; thiazides; beta blockers; or calcium channel blockers?
Well it’s better. It’s still not perfect, but yes, calcium channel blockers, correct answer.
Conclusions – Slide 49
So in conclusion, consistent with the Princeton III Consensus, all men should be asked about their sexual function regardless of their chief complaint. And if they have ED, determine their risk factors for cardiovascular disease. Oral therapies appear to be safe. And although there’s no conclusive data linking PDE5 as causing melanoma, sunscreen is still a good thing. Thank you.
ABOUT THE AUTHOR
Ryan P. Terlecki, MD, is a reconstructive urologist for Wake Forest Baptist Health, an academic Level 1 trauma center in Winston-Salem, North Carolina. His positions include Vice Chair and Associate Professor of Urology, Director of the Men’s Health Clinic, Director of Medical Student Education, and Fellowship Director for Reconstructive Urology. He is also the President of the North Carolina Urological Association. His publications cover multiple areas of trauma and reconstruction and his research is focused primarily on models of wound healing and regeneration in the lower genitourinary system. Dr. Terlecki completed two separate fellowships in reconstructive surgery following his residency, and is a member of the Society of Genitourinary Reconstructive Surgeons (GURS). Dr. Terlecki’s areas of expertise include urethral stricture disease, male sexual dysfunction, male incontinence, Peyronie’s disease, chronic testicular pain, hypogonadism, and infertility.